本帖最后由 老马 于 2013-5-15 15:04 编辑
Biomarkers Discovered That May Help Predict Response to Drugs Targeting KRAS-mutated NSCLC
April 7, 2013
http://www.aacr.org/home/public- ... he-news.aspx?d=3060
Effective targeted treatments for NSCLC with KRAS mutations are lacking.
MEK/PI3-kinase inhibitor combination is a promising treatment for this type of cancer.
Use of biomarkers could help guide treatment decisions.
WASHINGTON, D.C. — Scientists have identified biomarkers that may help predict whether patients with KRAS-mutated non-small cell lung cancer (NSCLC) will respond to concurrent treatment with an MEK inhibitor and a PI3 kinase inhibitor, a drug combination currently being investigated in ongoing clinical trials. The discovery was made as part of a study presented at the AACR Annual Meeting 2013, held in Washington, D.C., April 6-10, by Aaron N. Hata, M.D., Ph.D., a clinical fellow at the Massachusetts General Hospital in Boston.
Although several targeted therapies have been developed for patients with NSCLC, there are currently no proven targeted treatments for patients with NSCLC that harbors a KRAS mutation, which accounts for 20 percent to 25 percent of all NSCLC cases.
“Treatment with an MEK inhibitor and PI3 kinase inhibitor is a combination targeted therapy that may be effective for some patients with KRAS-mutant NSCLC, but it is not likely to be effective for all patients with this form of cancer,” said Hata. “We want to be able to know which patients are going to respond to this combination therapy so that we can identify them and tailor their treatment accordingly.”
To explore response to MEK and PI3 kinase inhibitors, Hata and colleagues studied a variety of NSCLC cell lines that all had mutated KRAS. They found that some of the cancer cell lines responded to the drug combination by undergoing a process of cell death called apoptosis, whereas others did not.
“Our results were not surprising from the standpoint that induction of cell death is known to be important for response of cancer cells to therapy,” Hata said. “What was surprising was the difference in apoptosis among the cell lines.”
Specifically, lack of a cell death response to the combination of MEK and PI3 kinase inhibitors correlated with the decreased expression of pro-cell death mediators and the upregulation of anti-cell death regulators.
“We found that three specific proteins predicted response,” Hata said. “Two of them, the BIM and PUMA proteins, induced cell death, and the third, the BCL-XL protein, inhibited cell death.”
In addition, prior research has shown that many KRAS-mutant lung cancers also have a mutation in the TP53 gene, and the protein that it generates, P53, is known to be involved in the cell death process. In this study, the researchers found that TP53 mutation status did not predict response to the MEK/PI3 kinase inhibitor combination, but it did affect how the cells underwent cell death.
“Our research so far has focused on human cancer cell lines,” Hata said. “We do not yet know if these correlations will hold true in patients.”
Ideally, Hata and his colleagues would like to determine whether the proteins they identified are predictive of patient response to MEK/PI3 kinase inhibitors in the clinic.
“The ultimate goal would be having the ability to measure levels of these proteins in patients before they go on treatment,” Hata said. “If they have favorable levels, that would tell us they are likely to respond to this treatment, and if they do not, it would be better to select a different treatment.” |
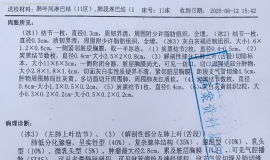
 父亲肺鳞癌,cT3N0M1a,ⅣA,脑转移
父亲2025年6月中旬因为头痛,一侧肢体不灵活入院,做了增强核磁,发现右侧额叶占位(3
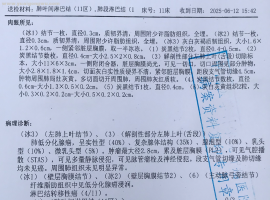
父亲肺鳞癌,cT3N0M1a,ⅣA,脑转移
父亲2025年6月中旬因为头痛,一侧肢体不灵活入院,做了增强核磁,发现右侧额叶占位(3
 老公刚刚54岁,确诊肺癌,手术中发现
各位朋友好。
度过了慌乱的一个月,有机会发现了这个论坛,如获至宝,说说我家
老公刚刚54岁,确诊肺癌,手术中发现
各位朋友好。
度过了慌乱的一个月,有机会发现了这个论坛,如获至宝,说说我家
 SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
 希望给没有阅读过的人一些体会
本文来自于此书,只是做一些摘抄,分享给深陷迷茫的人。文中观点真实与否,效果怎么
希望给没有阅读过的人一些体会
本文来自于此书,只是做一些摘抄,分享给深陷迷茫的人。文中观点真实与否,效果怎么
 L858R+S768I+TP53阿法替尼用药半年希
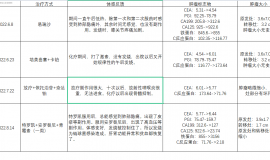
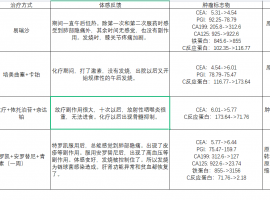
2023.11.23我父亲(63岁)因胸腔积液,呼吸困难,后背疼,声音沙哑入院。此前一个多月
L858R+S768I+TP53阿法替尼用药半年希
2023.11.23我父亲(63岁)因胸腔积液,呼吸困难,后背疼,声音沙哑入院。此前一个多月





 显身卡
显身卡